
Keratoconus
When your cornea changes shape — and glasses stop working — we have answers.
What Is Keratoconus?
Your cornea is supposed to be shaped like a smooth dome — like the front of a basketball. In keratoconus, that dome slowly thins out and starts to bulge forward into a cone shape. And when the front of your eye changes shape, light can't focus properly on your retina. The result? Blurry, distorted vision that glasses and regular contact lenses can't fully correct.
In my practice, I see this condition more often than most people expect. It typically starts in the late teens or early twenties — which is exactly why I take it seriously when a young patient keeps coming back with a prescription that won't stabilize. That's one of the first red flags.
Keratoconus affects roughly 1 in 375 to 1 in 2,000 people, depending on the population studied. It's more common than glaucoma in young adults, yet it's frequently missed — especially in patients who've only ever had basic vision screenings.
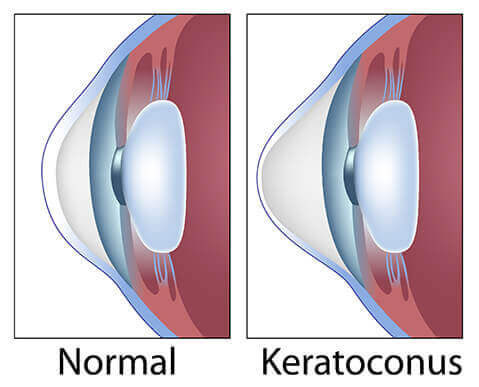
Left: Normal dome-shaped cornea. Right: Keratoconus — the cornea thins and bulges forward into a cone.
Symptoms & Warning Signs
Keratoconus doesn't announce itself with pain. It sneaks up on you. Here's what I tell patients to watch for:
Blurry or distorted vision
Straight lines look wavy or bent
Ghost images
Seeing double or multiple images from one eye
Halos & glare at night
Especially around headlights and streetlights
Light sensitivity
Bright lights feel uncomfortable or painful
Frequent prescription changes
New glasses every 6–12 months that never feel quite right
Eye rubbing
Chronic rubbing from allergies can accelerate progression
When to come in immediately
If you experience a sudden, dramatic worsening of vision in one eye — especially with pain or redness — this could be acute corneal hydrops, a rare complication of keratoconus where the cornea swells suddenly. Call us right away.
Causes & Risk Factors
We don't always know exactly why keratoconus develops in a specific person. But the research points to a few consistent patterns.
| Risk Factor | What We Know |
|---|---|
| Family history | 1 in 10 patients have a parent with keratoconus. If a first-degree relative has it, your risk is 15–67× higher. |
| Eye rubbing | Chronic, forceful rubbing — especially from allergies — is one of the strongest modifiable risk factors. It physically weakens corneal tissue over time. |
| Allergies & atopy | Eczema, asthma, and hay fever are all associated with keratoconus, largely because they drive eye rubbing. |
| Connective tissue disorders | Down syndrome, Marfan syndrome, and Ehlers-Danlos syndrome all increase risk. The cornea is connective tissue. |
| Age of onset | Most commonly diagnosed between ages 10–25. Progression typically slows after age 40. |
| UV exposure | Oxidative stress from UV light may contribute to corneal thinning. UV-blocking sunglasses matter. |
One thing I always ask new patients: do you rub your eyes a lot? A lot of folks with allergies have been rubbing their eyes since childhood without realizing the damage it can cause. If that's you, we need to talk about allergy management as part of your overall eye health plan.
How We Diagnose It
A standard eye chart test will not catch keratoconus. Neither will a basic vision screening at school or the pediatrician's office. To diagnose keratoconus, we need to look at the shape and thickness of your cornea — and that requires specialized equipment.
The most important tool is corneal topography — a non-contact scan that creates a color-coded map of your cornea's surface. Think of it like a topographical map of mountains and valleys. In a healthy eye, the map is smooth and symmetrical. In keratoconus, you'll see a characteristic "hot spot" — a steep, irregular area where the cone is forming. The warm colors (red, orange) indicate steeper, thinner areas.
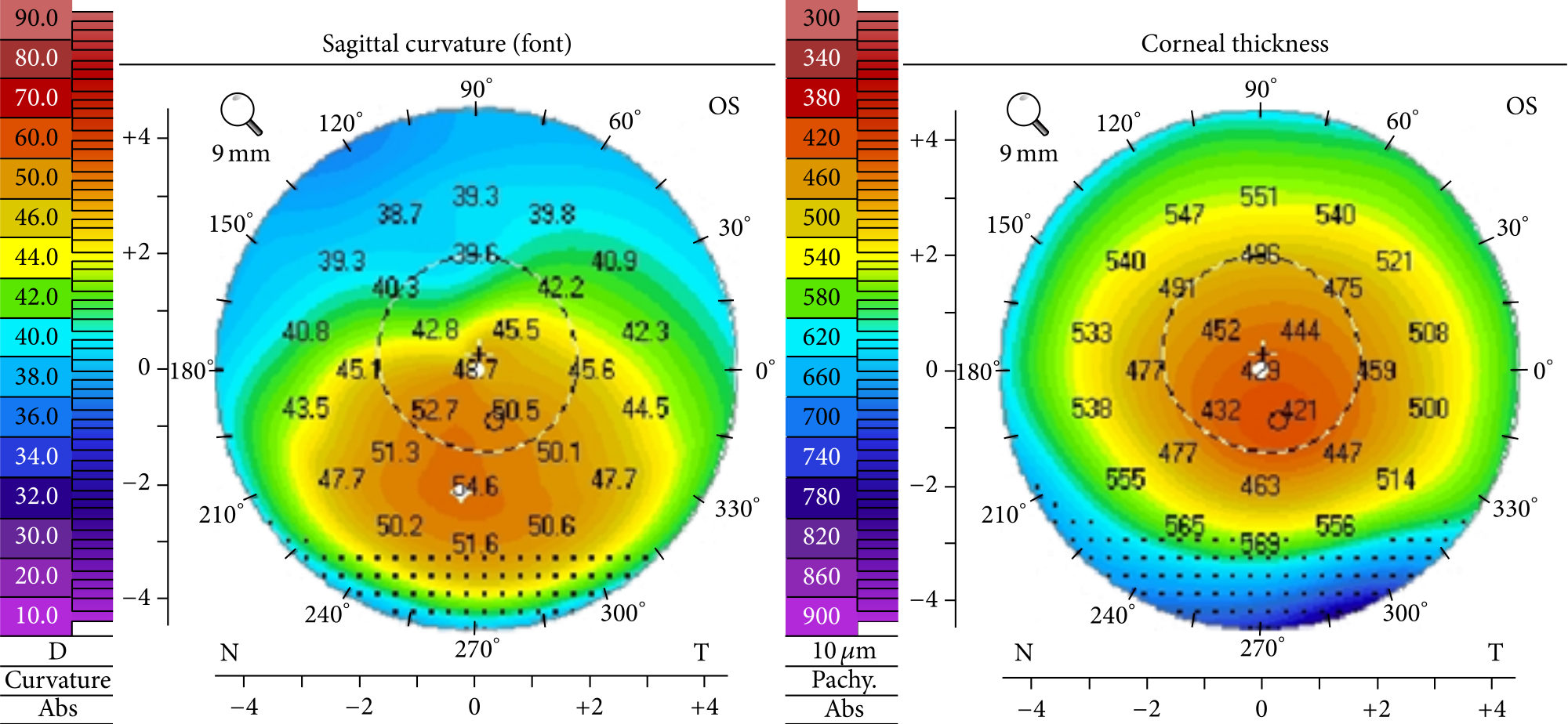
Corneal topography maps the shape and curvature of your cornea. The warm colors (red/orange) indicate the steep, irregular cone area characteristic of keratoconus.
We also use Scheimpflug imaging (like the Pentacam) to measure corneal thickness from front to back. This gives us a 3D picture of the entire cornea — not just the surface. It's how we catch early keratoconus before it causes noticeable vision problems.
If you've been told your prescription "just keeps changing" or that you have "irregular astigmatism," please come in for a full corneal evaluation. That's often the first sign something more is going on.
Stages of Keratoconus
Keratoconus is graded in stages using the Amsler-Krumeich classification. Understanding your stage helps us choose the right treatment.
| Stage | Corneal Shape | Vision Impact | Typical Treatment |
|---|---|---|---|
| Stage I (Mild) | Slight irregularity, mild steepening | Correctable with glasses or soft lenses | Monitoring, glasses or soft contacts |
| Stage II (Moderate) | Noticeable cone, increased steepening | Glasses less effective, distortion increases | RGP or scleral lenses, consider CXL |
| Stage III (Advanced) | Significant cone, corneal thinning | Significant distortion, halos, ghosting | Scleral lenses, CXL if still progressing |
| Stage IV (Severe) | Severe thinning, possible scarring | Severely impaired, may not correct fully | Scleral lenses, Intacs, or corneal transplant |
Why Regular Contacts Don't Work — And What Does
This is the question I get most often from newly diagnosed patients: "Can't I just wear my regular contacts?" Here's the thing — soft contact lenses are designed for a normal, spherical cornea. They're flexible, so they conform to whatever shape your eye is. That's great when your cornea is smooth. But in keratoconus, the lens just drapes over the cone like a wet cloth over a fist. It can't create a smooth optical surface, so your vision stays blurry and distorted.
Regular Soft Lenses
- • Flexible — conform to the irregular cone shape
- • Cannot create a smooth optical surface
- • Vision remains blurry and distorted
- • May feel comfortable but don't correct vision
- • Diameter: ~14mm
Rigid Gas Permeable (RGP)
- • Rigid — holds its shape over the cone
- • Creates a smooth front surface for light
- • Better vision than soft lenses
- • Can be uncomfortable; may pop out
- • Diameter: ~9–10mm
Scleral Lenses (Best Option)
- • Vaults completely over the entire cornea
- • Fluid reservoir fills the irregular gap
- • Crisp, stable vision — even in severe cases
- • Very comfortable; stays in place
- • Diameter: ~16–22mm
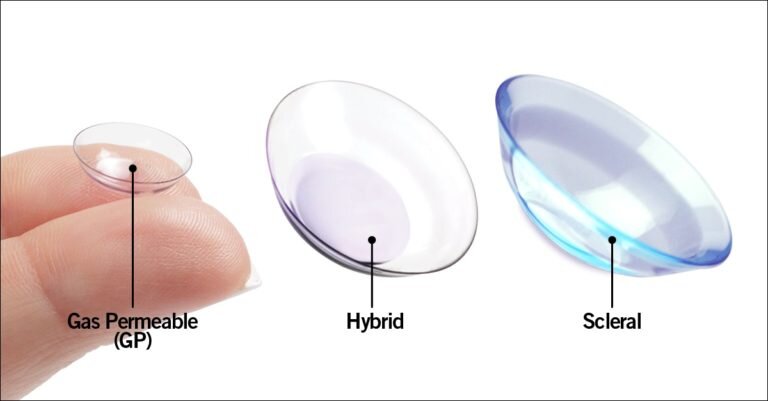
Size comparison: Gas Permeable (small, rigid), Hybrid, and Scleral (large) contact lenses. Scleral lenses are significantly larger and vault over the entire cornea.
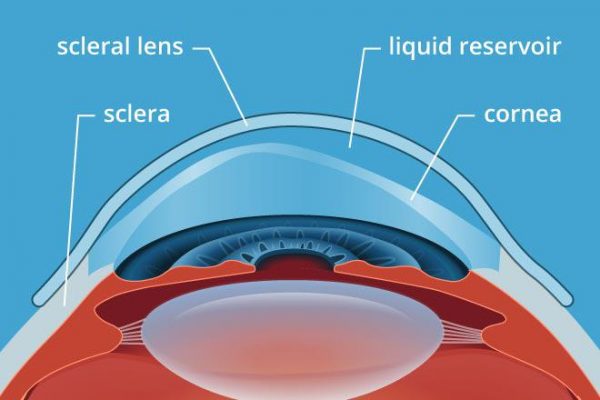
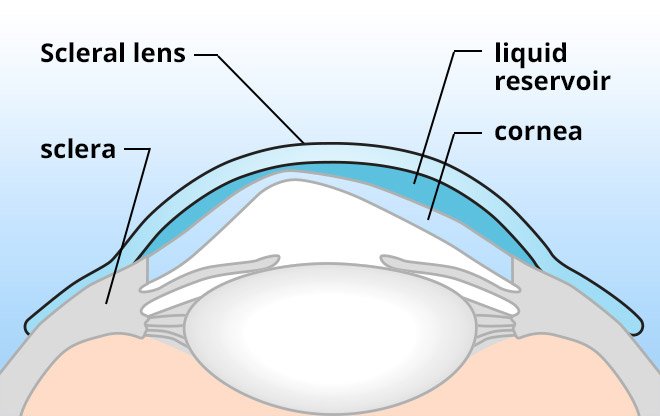
How scleral lenses work: the lens vaults completely over the irregular cornea and rests on the white of the eye (sclera). The fluid-filled space between the lens and cornea creates a smooth optical surface.
Real-world size comparison: 18mm scleral, 16mm scleral, standard soft lens, and gas permeable lens. The difference in size is dramatic — and intentional.
Treatment Options
There's no one-size-fits-all approach to keratoconus. Treatment depends on your stage, how fast it's progressing, and your lifestyle. Here's how I think about it.
Specialty Contact Lenses
Most CommonFor most patients, scleral lenses or RGP lenses are the primary treatment. They don't change the shape of your cornea — they just create a smooth surface for light to pass through, restoring sharp vision. Most patients with scleral lenses achieve 20/20 to 20/40 corrected vision.
Corneal Cross-Linking (CXL)
Stops ProgressionCXL uses riboflavin (vitamin B2) eye drops and UV light to create stronger bonds in the corneal collagen. It doesn't reverse the cone — but it stops it from getting worse. This is especially important for younger patients whose keratoconus is still progressing. The procedure takes about an hour and is done as an outpatient.
Intacs
Moderate CasesIntacs are tiny curved inserts placed just inside the outer edge of the cornea to flatten the cone shape. They can reduce astigmatism and improve how well contact lenses fit. The procedure takes about 15 minutes. They can also be removed if needed.
Corneal Transplant (DALK)
Severe Cases OnlyDeep Anterior Lamellar Keratoplasty (DALK) replaces the front layers of the cornea with donor tissue. It's reserved for Stage IV keratoconus with significant scarring when other treatments can no longer provide functional vision. Most patients still need specialty lenses after transplant.
Scleral Lenses: Our #1 Tool for Keratoconus
If I had to pick one treatment that has changed the most lives in my practice, it's scleral lenses. I've had patients come in who hadn't driven in years — their vision was that bad. After fitting them with sclerals, they're back behind the wheel. That's not an exaggeration. It happens regularly.
The fitting process is more involved than regular contacts. We start with a detailed corneal map, then order a custom trial lens. You come back, we put it in, check the fit under the slit lamp, and make adjustments. Most patients need 2–4 visits before we land on the perfect fit. It's worth every appointment.
What to Expect with Scleral Lenses
Keratoconus & Military Families
We're in Fayetteville — home of Fort Liberty, one of the largest military installations in the world. A significant portion of my patients are active duty service members, veterans, and their families. Keratoconus comes up more than you'd think in this community.
For those considering military service: keratoconus is generally a disqualifying condition for enlistment. But if it develops after you're already serving, there are often pathways for treatment and continued service — especially if the condition is stable and vision is correctable with specialty lenses.
TRICARE covers medically necessary keratoconus treatment in most cases, including specialty contact lenses and corneal cross-linking. Our team will verify your specific benefits before we start any treatment plan.
Fort Liberty Families — We've Got You
We understand the unique demands of military life — deployments, frequent moves, and the importance of maintaining vision readiness. We work with TRICARE and can coordinate care around your schedule. Call us at 910.426.3937.
Free Resource
Keratoconus Patient Checklist
Download our free checklist: 10 questions to ask your eye doctor if you think you may have keratoconus. Know what to look for, what tests to request, and what your options are.
Schedule a Keratoconus Evaluation →Frequently Asked Questions
Related Services at Eye Medics
References
- 1. Godefrooij DA, et al. "Age-specific incidence and prevalence of keratoconus." JAMA Ophthalmol. 2017;135(11):1232–1237.
- 2. Hashemi H, et al. "Global and regional estimates of prevalence of keratoconus." Cornea. 2020;39(2):263–270.
- 3. Woodward MA, et al. "Scleral lens use in the United States." Eye Contact Lens. 2016;42(6):e1–e3.
- 4. Hersh PS, et al. "Corneal collagen crosslinking for keratoconus and corneal ectasia: One-year results." J Cataract Refract Surg. 2011;37(1):149–160.
- 5. National Eye Institute — Keratoconus
- 6. NC Division of Public Health — Vision Program
Last reviewed: March 2026
Medical Disclaimer
This page is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The information provided here should not be used as a substitute for professional medical advice from a qualified eye care provider. Always consult with a licensed optometrist or ophthalmologist regarding any eye health concerns, symptoms, or treatment decisions.
Think You Might Have Keratoconus?
Don't wait for your vision to get worse. A corneal topography scan takes less than 5 minutes and can tell us exactly what's going on.